THYROID is an important endocrine gland of human body and plays vital role in the normal functioning of the body. It has important effects on glucose metabolism along with lipids and proteins and conversely can be affected by abnormal glucose metabolism.
Recently new research has found a strong link between type 2 diabetes and an increased risk of hypothyroidism, the most common type of thyroid disorder. It is the situation where the thyroid fails to make enough thyroid hormone to regulate the body's metabolism. The findings were presented at the American Association of Clinical Endocrinologists (AACE) 20th Annual Meeting and Clinical Congress in San Diego last month.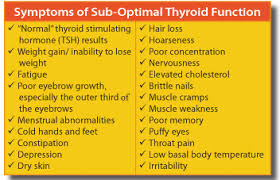
Recently new research has found a strong link between type 2 diabetes and an increased risk of hypothyroidism, the most common type of thyroid disorder. It is the situation where the thyroid fails to make enough thyroid hormone to regulate the body's metabolism. The findings were presented at the American Association of Clinical Endocrinologists (AACE) 20th Annual Meeting and Clinical Congress in San Diego last month.
Symptoms of underactive thyroid gland functioning, no matter what the cause, include fatigue, dry, coarse skin and hair, inability to tolerate cold weather, weight gain, hoarse voice, and heavy or irregular menstrual periods. The symptoms develop so slowly that sometimes people just think they are growing old prematurely.
Thyroid disorders (hypothyroidism or hyperthyroidism) and diabetes mellitus are quite common endocrinopathies (diseases of endocrine glands) seen in general population. Thyroid disorder in the general population is estimated to be 6.6%, while the prevalence in diabetic population has been estimated at 10.8%. The prevalence of sub-clinical (early stage) hypothyroidism is 5.4% and clinical hypothyroidism is 4.1%, while the prevalence of sub clinical hyperthyroidism is 5.8% and the clinical hyperthyroidism is 5.1%, the researchers noted.
The cross-sectional study comparing 1,848 adult patients with type 2 diabetes with 3,313 individuals without diabetes, showed the prevalence of hypothyroidism on the study group to be 5.7% compared with 1.8% in the control group (P ≤.0001).
Citing the Whickham survey, the researchers said thyroid function affected 6.6% of adults. A higher prevalence of abnormal TSH concentration in Type 2 diabetic patients (31%) was reported by Celani et al, they pointed out. In their study, sub-clinical hypothyroidism was detected in 11.66% of evaluated diabetic patients and hypothyroidism was evident in 35% of diabetic patients, which is a quite high ratio as compared to other reported data. “This may be because of only concentrating diabetes mellitus and its complications rather than thinking other diagnosis partly or misreporting by patients,” they noted.
“Although there is a recognized association between thyroid disease and diabetes, this association has been perceived mostly for type 1 diabetes. However, in type 2 diabetes, there is no consensus as to whether screening for hypothyroidism is necessary. We were surprised that the results showed an association that was this high,” said lead author Hector Eloy Tamez-Perez, MD, Autonomous University of Nuevo Leon, Monterrey, Mexico.
The study included patients who were enrolled in a private outpatient clinic in 2009, had a diagnosis of type 2 diabetes, and were treated with levothyroxine (Levothroid, Levoxyl, Synthroid, Tirosint, Unithroid), although patients with thyroid neoplasia (the process of abnormal and uncontrolled growth of cells. The product of neoplasia is a neoplasm, i.e. a tumor), panhypopituitarism (a deficiency involving all the hormonal functions of the pituitary gland), or have surgical complications of a multinodular goiter or a thyroid nodule were excluded.
It was found that around 10 per cent to 31 per cent of patients with type 2 diabetes had thyroid dysfunction, and that those with subclinical (early stage) hypothyroidism were the most common thyroid condition.
“So it is important to evaluate diabetic population regarding hypothyroidism whether clinical or sub-clinical, as one condition can worsen the other if left untreated by causing worsening control of diabetes mellitus, worsening dyslipidemias and causing diverse complications. Therefore, it is imperative to screen diabetic population regarding hypothyroidism. Moreover further studies on large scale should be planned to evaluate the magnitude of the disorder,” they concluded.
Popular Health Central columnist Dr Bill Quick, a physician living with diabetes, writes:
Thyroid disorders (hypothyroidism or hyperthyroidism) and diabetes mellitus are quite common endocrinopathies (diseases of endocrine glands) seen in general population. Thyroid disorder in the general population is estimated to be 6.6%, while the prevalence in diabetic population has been estimated at 10.8%. The prevalence of sub-clinical (early stage) hypothyroidism is 5.4% and clinical hypothyroidism is 4.1%, while the prevalence of sub clinical hyperthyroidism is 5.8% and the clinical hyperthyroidism is 5.1%, the researchers noted.
The cross-sectional study comparing 1,848 adult patients with type 2 diabetes with 3,313 individuals without diabetes, showed the prevalence of hypothyroidism on the study group to be 5.7% compared with 1.8% in the control group (P ≤.0001).
Citing the Whickham survey, the researchers said thyroid function affected 6.6% of adults. A higher prevalence of abnormal TSH concentration in Type 2 diabetic patients (31%) was reported by Celani et al, they pointed out. In their study, sub-clinical hypothyroidism was detected in 11.66% of evaluated diabetic patients and hypothyroidism was evident in 35% of diabetic patients, which is a quite high ratio as compared to other reported data. “This may be because of only concentrating diabetes mellitus and its complications rather than thinking other diagnosis partly or misreporting by patients,” they noted.
“Although there is a recognized association between thyroid disease and diabetes, this association has been perceived mostly for type 1 diabetes. However, in type 2 diabetes, there is no consensus as to whether screening for hypothyroidism is necessary. We were surprised that the results showed an association that was this high,” said lead author Hector Eloy Tamez-Perez, MD, Autonomous University of Nuevo Leon, Monterrey, Mexico.
The study included patients who were enrolled in a private outpatient clinic in 2009, had a diagnosis of type 2 diabetes, and were treated with levothyroxine (Levothroid, Levoxyl, Synthroid, Tirosint, Unithroid), although patients with thyroid neoplasia (the process of abnormal and uncontrolled growth of cells. The product of neoplasia is a neoplasm, i.e. a tumor), panhypopituitarism (a deficiency involving all the hormonal functions of the pituitary gland), or have surgical complications of a multinodular goiter or a thyroid nodule were excluded.
It was found that around 10 per cent to 31 per cent of patients with type 2 diabetes had thyroid dysfunction, and that those with subclinical (early stage) hypothyroidism were the most common thyroid condition.
“So it is important to evaluate diabetic population regarding hypothyroidism whether clinical or sub-clinical, as one condition can worsen the other if left untreated by causing worsening control of diabetes mellitus, worsening dyslipidemias and causing diverse complications. Therefore, it is imperative to screen diabetic population regarding hypothyroidism. Moreover further studies on large scale should be planned to evaluate the magnitude of the disorder,” they concluded.
Popular Health Central columnist Dr Bill Quick, a physician living with diabetes, writes:
Treatment for hypothyroidism is straight-forward: give the patient thyroid hormone replacement. How much thyroid hormone to give is about the only question: give too little, and the symptoms continue; give too much and the patient can become hyperthyroid. Physicians adjust the dose of thyroid hormone replacement by rechecking the TSH (thyroid stimulating hormone) level rather than judging by symptom levels: when the TSH is in the normal range, it can be assumed that the amount of thyroid hormone replacement therapy is appropriate.
Testing for hypothyroidism is easy to do, thyroid disease is common in the age group that has T2DM, treatment for hypothyroidism is easy and rewarding in relieving symptoms and decreasing the risk of future disease.
Lab tests for hypothyroidism are done using a standard blood sample, and include measurement of the TSH levels, thyroid hormone levels (called T3 and T4), and sometimes thyroid antibodies. In a patient with the symptoms, an elevated TSH level with simultaneous low levels of T3 and T4 are conclusive evidence that the thyroid gland is underactive. Indeed, a high level of TSH with normal levels of T3 and T4 are considered very suggestive evidence of impending hypothyroidism and worthy of treatment.
By the way, note the paradox: the TSH level is high in most underactive thyroid disorders. This is easy to understand when it is understood that TSH is made elsewhere, in the pituitary gland, and if the thyroid is failing to make its thyroid hormone, then the pituitary gland attempts to stimulate the thyroid to make more thyroid hormone, hence the TSH level goes up. For people without symptoms of hypothyroidism, measurement of the TSH level can be used as a screening test to look for early thyroid gland problems; sometime, it's also recommended that thyroid antibodies be part of the screening process.
The American Diabetes Association suggests for patients with T1DM that "TSH concentrations should be measured after metabolic control has been established. If normal, they should be re-checked every 1-2 years, or if the patient develops symptoms of thyroid dysfunction..." But there's no ADA recommendation for people with T2DM. The authors of the (Monterrey study) abstract (cited above) advised testing "similar to what occurs in type 1 diabetes."If you have diabetes, whether T1DM or T2DM, it seems reasonable that you should have your TSH level checked every year or two.
Natural treatment methods will put the woman in an optimal state of health, which can minimize the chance of having a miscarriage or a premature labor.
ReplyDelete